Alcohol MISUSE
Alcohol misuse accounts for
The Liver
- 1.5% of all premature deaths in England (8,367 deaths in 2012) (ONS, 2014).
- £3.5bn in costs to NHS annually (Department of Health using 2009/10 prices).
- Over 200,000 admissions to hospital in 2010/11 (Health & Social Care Information Centre, 2013).
- Affects all areas of society (including women, children and the elderly)
The Liver
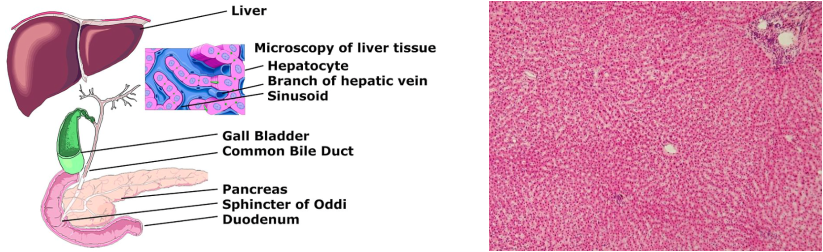
The liver (and associated organs) A healthy liver under a microscope
The liver's main roles are to filter toxins from the blood, help digest food by producing bile and regulating our blood sugar and cholesterol.
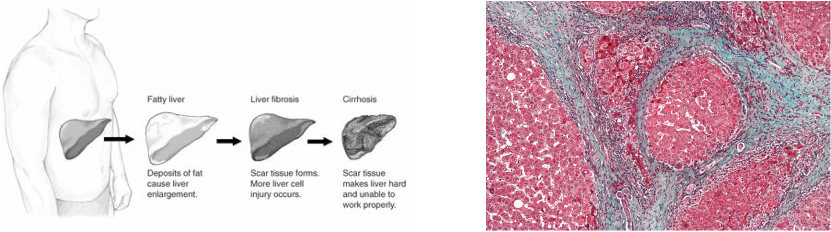
When the liver filters alcohol from the blood it's cells become damaged. They usually then renew and repair themselves but overuse of alcohol reduces this capacity to renew. This leads to more damage over time, which leads to reduced function. When the liver starts being damaged by alcohol it is called Alcohol Related Liver Disease (ARLD) and there are three stages:
AFLD
This is when fat builds up inside the liver cells. This can happen in days and usually has no symptoms. It might be found on blood tests which show abnormal liver enzymes or high fat levels. It is reversible if alcohol consumption is reduced or avoided.
Alcoholic Hepatitis
This usually occurs after longer term alcohol use but can occur after a single binge. In this condition the liver actually becomes inflamed and damaged. It is more common if the liver is already inflamed by viral hepatitis (B/C). Acute hepatitis is life threatening and needs urgent assessment. It presents with fever, jaundice, pain and deranged blood tests. Treatment is usually with high doses of steroids and vasodilators.
Cirrhosis
Cirrhosis is when the damage progresses to permanent scarring of the liver. Cirrhosis might, therefore, co-eixts with hepatitis. It results in deranged function of the liver and so has life threatening consequences. It is not reversible and the only treatment is to stop the damage (i.e. stop alcohol intake) and hope for a liver transplant.
When the liver filters alcohol from the blood it's cells become damaged. They usually then renew and repair themselves but overuse of alcohol reduces this capacity to renew. This leads to more damage over time, which leads to reduced function. When the liver starts being damaged by alcohol it is called Alcohol Related Liver Disease (ARLD) and there are three stages:
- Alcoholic Fatty Liver Disease (AFLD)
- Alcoholic Hepatitis
- Cirrhosis
AFLD
This is when fat builds up inside the liver cells. This can happen in days and usually has no symptoms. It might be found on blood tests which show abnormal liver enzymes or high fat levels. It is reversible if alcohol consumption is reduced or avoided.
Alcoholic Hepatitis
This usually occurs after longer term alcohol use but can occur after a single binge. In this condition the liver actually becomes inflamed and damaged. It is more common if the liver is already inflamed by viral hepatitis (B/C). Acute hepatitis is life threatening and needs urgent assessment. It presents with fever, jaundice, pain and deranged blood tests. Treatment is usually with high doses of steroids and vasodilators.
Cirrhosis
Cirrhosis is when the damage progresses to permanent scarring of the liver. Cirrhosis might, therefore, co-eixts with hepatitis. It results in deranged function of the liver and so has life threatening consequences. It is not reversible and the only treatment is to stop the damage (i.e. stop alcohol intake) and hope for a liver transplant.
|
The stages of liver damage
|
A liver affected by cirrhosis - the blue bands are irreversible scarring
|
Complications of Alcohol Related Liver Disease (ARLD)
Ethanol is the main alcohol in alcoholic drinks we consume. We measure the amount there is in units.
1 unit = 10ml of absolute alcohol = 1 single measure (25ml) of a 40% spirit.
When we drink alcohol the level in our blood rises. Depending on how high this level goes we experience different things. The level of alcohol in our blood differs between men and women, even if both have the same drink. This is because women have much less water in their bodies than men and so any alcohol consumed is less dilute. This is why the recommended safe drinking limits differ between genders. The recommended safe limits on alcohol consumption are recommended from the Royal Colleges of General Practitioners, Physicians & Psychiatrists and the BMA. They are based on how likely physical harm (excluding accidents) is likely to occur and they are as follows:
The Department of Health's recommendation is a little less stringent and, arguably, more vague. It suggests men should not 'regularly' drink more than 3-4 units per day (2-3 units for women).
- Portal hypertension - when the veins coming to the liver get blocked
- Oesophageal varices - risk of fatal bleeding from the throat
- Ascites - build of of fluid in the abdomen
- Spontaneous peritonitis - life threatening infection
- Hepatic encephalopathy - confusion caused by excess toxins affecting the brain
- Liver cancer - the risk of liver cancer increases in those with cirrhosis
Ethanol is the main alcohol in alcoholic drinks we consume. We measure the amount there is in units.
1 unit = 10ml of absolute alcohol = 1 single measure (25ml) of a 40% spirit.
When we drink alcohol the level in our blood rises. Depending on how high this level goes we experience different things. The level of alcohol in our blood differs between men and women, even if both have the same drink. This is because women have much less water in their bodies than men and so any alcohol consumed is less dilute. This is why the recommended safe drinking limits differ between genders. The recommended safe limits on alcohol consumption are recommended from the Royal Colleges of General Practitioners, Physicians & Psychiatrists and the BMA. They are based on how likely physical harm (excluding accidents) is likely to occur and they are as follows:
- MEN should drink no more than 21 units per week (less than 4 units per day), ideally with 2-3 alcohol free days in a week;
- WOMEN should drink no more than 14 units per week (less than 3 units per day) ideally with 2-3 alcohol free days in a week;
- PREGNANT WOMEN should avoid alcohol in the first trimester but it is likely to be safe to drink 1-2 units at a time on a maximum of 2 days per week thereafter (RCP, 2011).
The Department of Health's recommendation is a little less stringent and, arguably, more vague. It suggests men should not 'regularly' drink more than 3-4 units per day (2-3 units for women).
What Constitutes Dangerous Drinking?
Having explored some facts about alcohol and it's affect on the liver, let's move on to consider how alcohol problems might be managed in the community.
- LOW RISK drinking is a pattern that follows the suggested limits above
- HAZARDOUS DRINKING is intake that is likely to increase the risk of developing alcohol related harm. It is when MEN drink 22-50 units a week and WOMEN 15-35 units a week.
- HARMFUL DRINKING is intake that is associated with alcohol-related harm. For MEN that is >50 units a week and for WOMEN >35 units a week.
- strong compulsion/desire to drink
- diffculty in controlling the onset or termination of drinking
- a withdrawal state on cessation of drinking
- increasing tolerance to alcohol so that increasing amounts are needed to achieve similar effects
- progressive neglect of other interests
- persistent use of alcohol despite clear evidence and awareness of the harm it is causing
Having explored some facts about alcohol and it's affect on the liver, let's move on to consider how alcohol problems might be managed in the community.

|

|
References
With credit to Dr Zana Khan (GP, Kings Health Partnership, London) for letting us reproduce this material.
Department of Health. The cost of alcohol harm to the NHS in England. 2003 (updated 2008). Available in the web archives at - http://www.dh.gov.uk/en/Consultations/Liveconsultations/DH_086412?IdcService=GET_FILE&dID=169373&Rendition=Web. This update has since been updated to reflect unit costs of 2009/10, giving the figure of £3.5bn.
Health and Social Care Information Centre. Statistics on Alcohol - England. 2013. http://www.hscic.gov.uk/catalogue/PUB10932
Morgan M Y, Ritson E B. Alchol and Health (5th edition. The Medical Council on Alcohol. London. 2010.
National Treatment Agency for Substance Misuse. Alcohol Treatment in England 2011-12. 2013. http://www.nta.nhs.uk/uploads/alcoholcommentary2013final.pdf
Office for National Statistics. Alcohol-related deaths in the United Kingdom registered in 2012. 2014. http://www.ons.gov.uk/ons/dcp171778_353201.pdf
Royal College of Physicians. The evidence base for alcohol guidelines. 2011. http://www.publications.parliament.uk/pa/cm201012/cmselect/cmsctech/writev/1536/ag22.htm
With credit to Dr Zana Khan (GP, Kings Health Partnership, London) for letting us reproduce this material.
Department of Health. The cost of alcohol harm to the NHS in England. 2003 (updated 2008). Available in the web archives at - http://www.dh.gov.uk/en/Consultations/Liveconsultations/DH_086412?IdcService=GET_FILE&dID=169373&Rendition=Web. This update has since been updated to reflect unit costs of 2009/10, giving the figure of £3.5bn.
Health and Social Care Information Centre. Statistics on Alcohol - England. 2013. http://www.hscic.gov.uk/catalogue/PUB10932
Morgan M Y, Ritson E B. Alchol and Health (5th edition. The Medical Council on Alcohol. London. 2010.
National Treatment Agency for Substance Misuse. Alcohol Treatment in England 2011-12. 2013. http://www.nta.nhs.uk/uploads/alcoholcommentary2013final.pdf
Office for National Statistics. Alcohol-related deaths in the United Kingdom registered in 2012. 2014. http://www.ons.gov.uk/ons/dcp171778_353201.pdf
Royal College of Physicians. The evidence base for alcohol guidelines. 2011. http://www.publications.parliament.uk/pa/cm201012/cmselect/cmsctech/writev/1536/ag22.htm
