Personality Disorders

Feedback obtained from primary care workers highlighted some uncertainty and a relative lack of confidence when it came to understanding and managing patients who have personality disorders.
The DSM IV defines a personality disorder (generally) as being "an enduring pattern of inner experience and behaviour the deviates markedly from the expectations of the individual's culture. This pattern is manifested in two (or more) of the following areas:
It then goes on to group personality disorders into three categories, A, B and C.
Group A is the 'odd' type. People with these disorders have difficulty relating to others:
Group B is the 'dramatic, emotional and erratic' type. People with this disorders have difficulty regulating extremes of feelings.
Group C is the 'anxious and fearful' type. People with these disorders have difficulty controlling sometimes overwhelming fear and anxiety.
Personality disorders are common and it is estimated that 1 in 20 adults in the UK have the features of at least one. They often emerge in adolescence and early adulthood and many follow a chronic relapsing and remitting course, with periods of stability. Many people overcome them completely.
There is no licensed 'treatment' (certainly not medication) for personality disorders. Forms of talking therapies such as psychodynamic therapy, cognitive-behavioural therapy and interpersonal therapy can be considered and clinical trials continue into different forms of treatment. (NICE, 2009).
Why is Personality Disorder Important in Homeless Healthcare?
Personality disorders affect all populations but there is an extensive body of literature supporting the hypothesis that mental health issues are more common amongst homeless patients (Fazel et al, 2008). Studies in the UK have shown that 59-66.7% of homeless people have features of at least one personality disorder although relatively few of those are formally diagnosed (Murphy et al, 2002; Middleton, 2008). Other studies have highlighted how a label of personality disorder can be stigmatising and make clinical staff believe the patient is harder to treat (Newton-Howes et al, 2008). Even nurses working in specialist forensic mental health units find patients with personality disorder more difficult to treat and are pessimistic about any treatment outcomes (Alexander et al, 2000). It is little wonder then, it seems, that a health care professional working alone can feel helpless and isolated when trying to help a patient with a personality disorder.
Of course, this website cannot provide the answers but there are, thankfully, useful strategies in the form of 'DO's and DON'TS' that can help ease the pressure and make difficult consultations more rewarding. These are shown below and all credit goes to the Thames Valley Initiative:
The DSM IV defines a personality disorder (generally) as being "an enduring pattern of inner experience and behaviour the deviates markedly from the expectations of the individual's culture. This pattern is manifested in two (or more) of the following areas:
- Cognition (i.e., ways of perceiving and interpreting self, other people and events)
- Affectivity (i.e., the range, intensity, liability, and appropriateness of emotional response)
- Interpersonal functioning
- Impulse control"
It then goes on to group personality disorders into three categories, A, B and C.
Group A is the 'odd' type. People with these disorders have difficulty relating to others:
- Paranoid type - express irrational suspicion and mistrust
- Schizoid type - exhibit lack of interest and detachment from social relationships
- Schizotypal type - show extreme discomfort in interacting socially and distorted cognitions/perceptions
Group B is the 'dramatic, emotional and erratic' type. People with this disorders have difficulty regulating extremes of feelings.
- Antisocial type - exhibit a disregard and violation of the rights of others and a lack of empathy
- Borderline type - exhibit instability in relationships, self image, self identity and are commonly impulsive self harmers
- Histrionic - exhibit attention seeking behaviours and extreme emotions
- Narcissistic - show grandiosity, a need for admiration and a lack of empathy
Group C is the 'anxious and fearful' type. People with these disorders have difficulty controlling sometimes overwhelming fear and anxiety.
- Avoidant type - exhibit social isolation, feeling of inadequacy and extreme sensitivity to negative outcomes
- Dependent type - have a need to be cared for by others
- Obsessive-Compulsive type - follow rigid rules and exhibit perfectionism and control to the satisfaction and exclusion of activities and friendships (DSM-IV, 2000).
Personality disorders are common and it is estimated that 1 in 20 adults in the UK have the features of at least one. They often emerge in adolescence and early adulthood and many follow a chronic relapsing and remitting course, with periods of stability. Many people overcome them completely.
There is no licensed 'treatment' (certainly not medication) for personality disorders. Forms of talking therapies such as psychodynamic therapy, cognitive-behavioural therapy and interpersonal therapy can be considered and clinical trials continue into different forms of treatment. (NICE, 2009).
Why is Personality Disorder Important in Homeless Healthcare?
Personality disorders affect all populations but there is an extensive body of literature supporting the hypothesis that mental health issues are more common amongst homeless patients (Fazel et al, 2008). Studies in the UK have shown that 59-66.7% of homeless people have features of at least one personality disorder although relatively few of those are formally diagnosed (Murphy et al, 2002; Middleton, 2008). Other studies have highlighted how a label of personality disorder can be stigmatising and make clinical staff believe the patient is harder to treat (Newton-Howes et al, 2008). Even nurses working in specialist forensic mental health units find patients with personality disorder more difficult to treat and are pessimistic about any treatment outcomes (Alexander et al, 2000). It is little wonder then, it seems, that a health care professional working alone can feel helpless and isolated when trying to help a patient with a personality disorder.
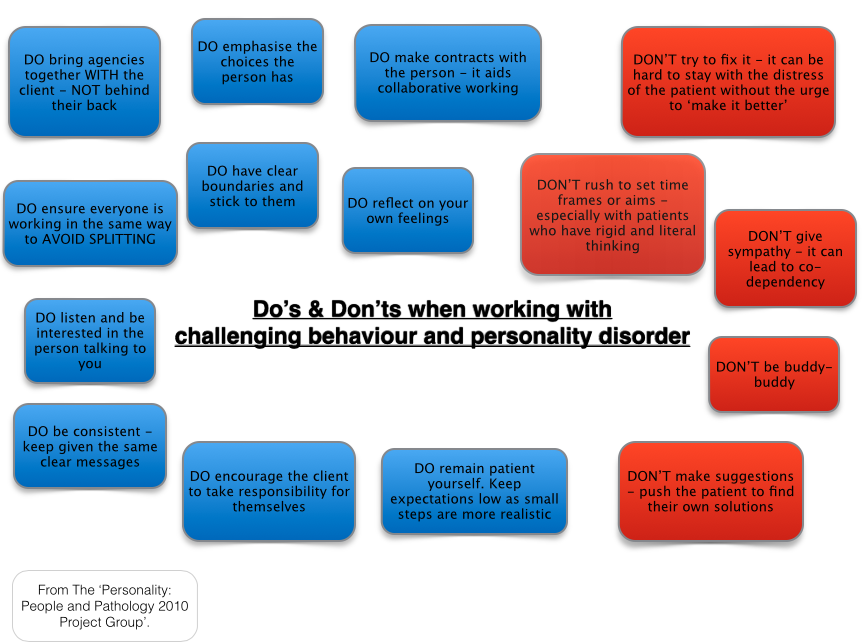
Of course, this website cannot provide the answers but there are, thankfully, useful strategies in the form of 'DO's and DON'TS' that can help ease the pressure and make difficult consultations more rewarding. These are shown below and all credit goes to the Thames Valley Initiative:
There are many foundations and website offering support relating to personality disorders but for more information and educational resources go to:
- NHS Choices Website - an excellent landing page with further explanation and very useful links
- The Thames Valley Initiative - offers training to all walks of healthcare professional about personality disorders and communication skills with the input of patients who have completed complex needs therapy.

|

|
References
Alexander J et al. Factors underlying and maintaining nurses' attitudes to patients with severe personality disorder - Final report to the National Forensic Mental Health R&D.City University of London. 2000. http://www.kcl.ac.uk/ioppn/depts/hspr/research/ciemh/mhn/projects/personalitydisorder/spd.pdf
Diagnostic and Statistical Manual of Mental Disorders - 4th Edition (text revised). American Psychiatric Association. 2000.
Hazel S, Khosla V, Doll H, Geddes J. The Prevalence of Mental Disorders among the Homeless in Western Countries: Systematic Review and Meta-Regression Analysis. 2008. DOI: 10.1371/journal.pmed.0050225.
Middleton R. (2008). Brokering Realities - Community Links. The Leeds Personality Disorder Clinical Network.
National Institute for Health and Care Excellence. Borderline Personality Disorder: Treatment and Management. Guidance CG78 (2009). https://www.nice.org.uk/guidance/cg78/chapter/1-guidance.
National Institute for Healthcare & Clinical Excellence. Guidance on commissioning stepped care for common mental health disorders (Guidance CMG41). 2001. http://publications.nice.org.uk/commissioning-stepped-care-for-people-with-common-mental-health- disorders-cmg41/3-a-stepped-care-approach-to-commissioning-high-quality-integrated-care-for- people-with-common.
Newton-Howes G, Weaver T, Tyrer P. Attitudes of staff towards patients with personality disorder in community mental health teams. Aust N Z J Psychiatry. 2008 Jul;42(7):572-7. doi: 10.1080/00048670802119739.
Alexander J et al. Factors underlying and maintaining nurses' attitudes to patients with severe personality disorder - Final report to the National Forensic Mental Health R&D.City University of London. 2000. http://www.kcl.ac.uk/ioppn/depts/hspr/research/ciemh/mhn/projects/personalitydisorder/spd.pdf
Diagnostic and Statistical Manual of Mental Disorders - 4th Edition (text revised). American Psychiatric Association. 2000.
Hazel S, Khosla V, Doll H, Geddes J. The Prevalence of Mental Disorders among the Homeless in Western Countries: Systematic Review and Meta-Regression Analysis. 2008. DOI: 10.1371/journal.pmed.0050225.
Middleton R. (2008). Brokering Realities - Community Links. The Leeds Personality Disorder Clinical Network.
National Institute for Health and Care Excellence. Borderline Personality Disorder: Treatment and Management. Guidance CG78 (2009). https://www.nice.org.uk/guidance/cg78/chapter/1-guidance.
National Institute for Healthcare & Clinical Excellence. Guidance on commissioning stepped care for common mental health disorders (Guidance CMG41). 2001. http://publications.nice.org.uk/commissioning-stepped-care-for-people-with-common-mental-health- disorders-cmg41/3-a-stepped-care-approach-to-commissioning-high-quality-integrated-care-for- people-with-common.
Newton-Howes G, Weaver T, Tyrer P. Attitudes of staff towards patients with personality disorder in community mental health teams. Aust N Z J Psychiatry. 2008 Jul;42(7):572-7. doi: 10.1080/00048670802119739.
