Difficult Consultations
To get the most from this module we strongly recommend doing the modules on PERSONALITY DISORDERS and ADDICTION TO PRESCRIPTION MEDICATION first. Both of these modules highlight models and principles of communicating in difficult circumstances. In this module these ideas will be reinforced by looking at how it is possible to still be patient centred in those difficult situations where it might not be possible to be patient pleasing.
Patient Centred vs Patient Pleasing Care
Ensuring a positive patient experience is one of the 5 domains of the NHS Outcomes Framework (NHS Outcomes Framework 2014/15). The NHS constitution itself also reinforces the commitment that there be 'no decision about me without me', firmly putting the patient at the centre of their care. What then, is a primary care health professional to feel if they genuinely believe that what the patient wants in the short term is not in their best interests in the long term? When is there a difference between being patient centred and purely patient pleasing? The concepts of patient autonomy and choice have always had to be balanced by the facts that resources are not limitless and that there is no 'right' to any particular treatment, only a right of 'access' to healthcare.
Conflict is an uncomfortable situation for most but can be especially difficult if what a patient and a healthcare professional hope to achieve are totally different. Some examples that might be experienced in primary care include:
Homeless populations often do not hold their general health as a top priority - they may have more immediate needs such as housing or may struggle with a substance dependence. This need to 'live in the immediate present' may translate into the intermittent use of primary health services for only what is perceived to be the immediate need (Quilgars and Pleace, 2003). The immediate problem might be related to mental or physical health, a request for detoxification from substances or, rarely, be a presentation in an attempt to secure addictive prescription medications to use personally or even divert illicitly for financial purposes.
In these situations the immediate perceived needs of the patient may not match with the agenda and perceived needs of the health care worker. For example, let's use a real life example where somebody presents in a crisis as matters outside of the surgery have caused their mental health to destabilise and as a result they have begun using illicit drugs.
Patient Centred vs Patient Pleasing Care
Ensuring a positive patient experience is one of the 5 domains of the NHS Outcomes Framework (NHS Outcomes Framework 2014/15). The NHS constitution itself also reinforces the commitment that there be 'no decision about me without me', firmly putting the patient at the centre of their care. What then, is a primary care health professional to feel if they genuinely believe that what the patient wants in the short term is not in their best interests in the long term? When is there a difference between being patient centred and purely patient pleasing? The concepts of patient autonomy and choice have always had to be balanced by the facts that resources are not limitless and that there is no 'right' to any particular treatment, only a right of 'access' to healthcare.
Conflict is an uncomfortable situation for most but can be especially difficult if what a patient and a healthcare professional hope to achieve are totally different. Some examples that might be experienced in primary care include:
- a debatable request for sickness certification
- request to postpone court appearances on the grounds of anxiety over the result (which may only continue the cycle of anxiety)
- request for possibly inappropriate medications
- request for possibly inappropriate referrals to secondary care
Homeless populations often do not hold their general health as a top priority - they may have more immediate needs such as housing or may struggle with a substance dependence. This need to 'live in the immediate present' may translate into the intermittent use of primary health services for only what is perceived to be the immediate need (Quilgars and Pleace, 2003). The immediate problem might be related to mental or physical health, a request for detoxification from substances or, rarely, be a presentation in an attempt to secure addictive prescription medications to use personally or even divert illicitly for financial purposes.
In these situations the immediate perceived needs of the patient may not match with the agenda and perceived needs of the health care worker. For example, let's use a real life example where somebody presents in a crisis as matters outside of the surgery have caused their mental health to destabilise and as a result they have begun using illicit drugs.
|
The Patient's Immediate Issues/Concerns
I need help with my mental health as I can't cope with feeling like this anymore. I want to detox off drugs (alcohol and heroin) again but can't do that unless my mental health is better or I'm in some kind of support. I need money to fund my shelter arrangements and dependence issues. I distrust figures of authority. This has become my immediate priority so I feel something needs to be done now. These issues might be presented as a request or demand to be admitted for a detox to hospital OR if that fails to be issued with sedating medications such as benzodiazepines in order to reduce withdrawal effects or to create income. |
The Presciber's General Issues/Concerns
This patient clearly has chronic issues with their mental health and substance misuse - these will affect each other. I'm note sure if I can access detox services immediately. Our mental health services will be reluctant to get involved if substance misuse is involved. I feel uncomfortable prescribing benzodiazepines as I feel unfamiliar with this patient and the health risks of respiratory depression in conjunction with opiates and the risk of the drugs being diverted for illegal sale is high. If I do nothing than I have not helped the patient and, at worst, could have damaged their relationship with health services further - they may not come back for other important issues. If I agree to prescribe unsuitable medications I am keeping them in a vicious cycle of harm and put myself at clinical risk as a prescriber. This patient's personality disorder means they might react badly to obstruction and conflict from figures of authority. These issues will manifest as a conflict of interests, which could understandably cause feelings of isolation, helplessness, frustration, anger and anxiety. |
In the above real life situation it is clear to see that doing exactly what the patient WANTS (immediate detox OR benzodiazepine prescription) may not be possible or desirable from a GP's point of view. However doing NOTHING could have very negative consequences on the patient's relationship with the health services and their mental health. It almost seems inevitable that both parties will leave the situtaiton with a sense of conflict, anxiety and stress.
So how can one 'say no' to those requests whilst still moving forward? One possibility lies within Longstaff and Schafer's model for dealing with addiction to prescription only medication. A copy of that model is shown below.
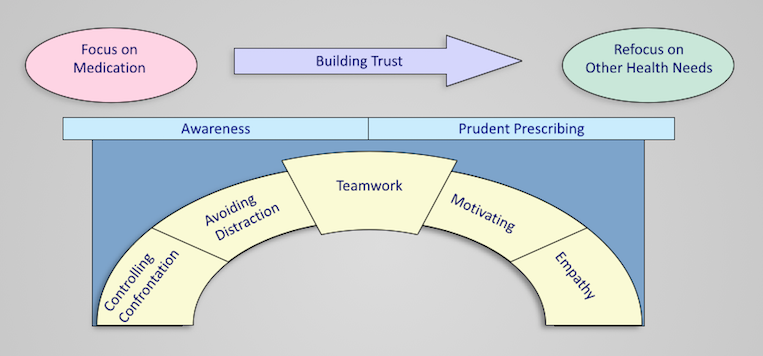
Although the pink starting point in this model explicitly focuses on prescription medication this might be replaced with an issue from our difficult situation above. The model highlights how you cannot deal with everything in one appointment and you may need to start at a point f immediate patient concern, then begin building a trusting and honest rapport with the patient so that the focus can be shifted onto the bigger picture: a process that is underpinned by the 5 domains in the arch.
If you haven't already seen the details about this model then GO HERE.
There are no right or wrong answers when it comes to the scenario above but using the learning points from the discussion about handling personality disorders and using Longstaff & Schafer's model the consultation might hopefully go something like this:
If you haven't already seen the details about this model then GO HERE.
There are no right or wrong answers when it comes to the scenario above but using the learning points from the discussion about handling personality disorders and using Longstaff & Schafer's model the consultation might hopefully go something like this:
|
Patient
"I can't take it anymore - I need a detox straight away" "I'm using heroin again and I just need to come off it now - I can't afford it and it's messing things up. I don't want to go back to the drugs service as it wasn't helpful last time, I just need to go to hospital or get into detox to get clean and I'll be ok" "So you can't help then? Well I'm going to need my prescription that the other doctor gave me last week for the diazepam then because I can't cope with the withdrawals and I can't carry on like this." |
Doctor
"I can see you're quite distressed, tell me, what's led up to this point?" "I understand. What if we can't get you into hospital for that reason straight away?" "Ok, I'm hearing that you need to change your situation quite quickly. What I can't do is get you admitted to a hospital immediately for that but what I can do is try and help in some other ways. I might not do things the same way as the other doctor so I'm not saying I definitely can or can't give you any benzo's today but I'd really like to get to know what's going on a little bit more" |
Area of model being used
Empathy Awareness (of local services) Prudent Prescribing Avoiding Distraction Trying to Build Trust |
It would hopefully be possible to build from this point in the consultation to gain more information, possibly deliver some basic harm reduction advice and arrange a clear follow up plan in order to try and maintain momentum. It would be vitally important to document or communicate this plan with any other members of the team who might involved in the future, including other doctors and allied services.
It might be appropriate to prescribe a short course of benzodiazepines in this situation, perhaps with the contract that it could be done on the proviso that the patient tries to engage with the community drug services and clearly stating it would be reducing dose or limited script. It might also be appropriate not to do so - benzodiazepines are quite easily available illicitly on the streets whether you prescribe them or not. It would be important to give harm reduction advice about reducing or stopping opiate use with concurrent benzo's and not taking the medication or the drugs alone in case of problems.
In the patient's next visit (hopefully with you) you might try to move things forward to include BBV screening, motivational interviewing and a gradual refocusing onto the bigger picture, such as housing status, general physical and mental health and even possibly employment. You cannot fix all of the problems but even if nothing else comes of this period of interaction with primary care other than Hepatitis B vaccination then, actually, significant harms have been averted. Remember that drug misuse is often a chronic, relapsing and remitting condition that cannot be cured in a s ingle consultation.

|

|
References
NHS Outcomes Framework. HM Government 2014/15 - https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256456/NHS_outcomes.pdf
Quilgars D, Pleace N. Delivering Healthcare to Homeless People: An Effectiveness Review. University of York for NHS Scotland. 2003. https://pure.york.ac.uk/portal/files/15515481/PDF_of_final_HEBS_report.pdf
NHS Outcomes Framework. HM Government 2014/15 - https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256456/NHS_outcomes.pdf
Quilgars D, Pleace N. Delivering Healthcare to Homeless People: An Effectiveness Review. University of York for NHS Scotland. 2003. https://pure.york.ac.uk/portal/files/15515481/PDF_of_final_HEBS_report.pdf
